
Photo Courtesy of Kelsey Savage & John Woods, Real Talk
On paper, Alison Klein is a serious academic with a master’s in interdisciplinary studies focused on adult education and disability. Meet her at one of the Real Talk’s free public events (affectionately known as “pizza parties”), and she’ll be the first to greet you as a peer facilitator and make a joke—sometimes with anatomically correct models at the ready.
“I go, ‘Look, a present’, and then just walk away,” says Klein with a smile. “I have kind of a funny side.”
Founded and managed by sexual health educator John Woods, Real Talk is an initiative based in Metro Vancouver that supports people with intellectual and developmental disabilities (IDD). Woods has worked in community living spaces, schools, and sexual health organizations since the early ’90s, both in Canada and in London, UK. He saw the urgent need for sex education tailored to the IDD community, and a slew of intersectional barriers rooted in eugenics. Now, in between pizza parties and Q&As, Real Talk works with the community living sector to support providers and those with cognitive disabilities.
“Step five is getting the public to acknowledge and affirm that folks with intellectual disabilities could be LGBTQ,” explains Kelsey Savage, Real Talk’s project developer. “Step zero is the general population believing that folks with intellectual disabilities have a sexuality at all.”
Since its founding in 2017, Real Talk has grown to include both certified sexual health educators and peer facilitators with lived experience, ensuring its initiatives are driven by community needs. While the disability rights rallying cry “nothing about us without us” has existed for decades, Real Talk remains one of the few accessible sex-positive resources that centre self-advocacy. It provides an extensive library of YouTube videos addressing common questions around sexuality and disability. Savage also oversees Connecting Queer Communities (CQC), a social group for 2SLGBTQIA+ folks with cognitive disabilities to connect across the Lower Mainland both in person and online. People often attend both Real Talk and CQC events, and several have joined Klein as peer facilitators themselves. As facilitators, honouring education and community could mean helping someone explain orgasms to their partner one day, and being with someone’s deepest traumas the next.
“It’s happened a number of times at our events, where people have discovered they’ve been taking birth control and it’s been called a vitamin, or they’ve had an IUD and they didn’t consent to it,” says Savage. “There’s already a lot in the room before you step into it.”
As Real Talk works across communities to expand its outreach, what’s needed to ensure the future of good sexual health education is clear: government-sponsored education and publicly funded accommodations and support so people with cognitive disabilities have an equitable pathway to become sexual health educators. “I want to ideally work myself out of a job,” teases Savage.
“Earlier, I was mostly around staff and disconnected from my community,” Klein says. “I hope Real Talk is a starting point, and that sex education can be taught in schools to kids from all different backgrounds, so they all have a frame of reference [for] each other.”
]]>
Collage by Valerie Thai
Isabella Calahoo-Zeller was attending eighth grade in Alberta when she received sex education for the first time. It consisted of a YouTube video about consent, and not much else. “We didn’t really get much on what a penis looks like, or what a vulva looks like,” Calahoo-Zeller says. “We never got the birth video that you hear so much about. So for me, I was like, what is this?”
Calahoo-Zeller is one of many young people in Alberta, and across Canada, who have been left wanting more from the sex ed experience offered in schools. Research by the Sex Information & Education Council of Canada (SIECCAN) has shown that 82.5 percent of young people across Canada see sex ed as a basic right for all.
These results come at a time when political and popular support for sex education seems to be shifting. Across the country, some parents, who claim to be advocating for parental rights, have been extremely vocal in their distaste for comprehensive sex ed, especially content focused on 2SLGBTQIA+ identities. According to Statistics Canada, about four percent of the population identifies as 2SLGBTQIA+. This means that if queer and trans-related content is left out of sex ed, many young Canadians won’t be receiving essential information about their health.
In Alberta, Saskatchewan, and New Brunswick, trans and nonbinary young people’s rights in the education space are on a backslide. New policies by the United Conservative Party, the Saskatchewan Party, and the Progressive Conservative Party respectively around the use of changed names and pronouns, as well as sex-ed access, are increasing the number of hoops through which young people have to jump to be recognized as their authentic selves and access resources made to support them.
“You’re already struggling in surviving to be yourself. How can you ask for help when the help doesn’t want to help you, right? I think it’s really a struggle right now being a trans person,” says Calahoo-Zeller, who is Two Spirit.
The benefits of receiving comprehensive sexuality education have been proven by science, and they’re not just about healthy and safe sex. From a violence prevention perspective, sex ed is key because it builds knowledge and understanding of bodily autonomy. It can be the first place children who are being abused learn that what’s happening to them is not okay. The health and safety aspect of sexuality education is essential, but that’s no less true of learning about gender identity, self-expression, and the full spectrum of human relationships.
“Historically, sexual health education focused on issues related to problem prevention. It has been focused on the needs of heterosexual, cisgender, white youth primarily, and focused on preventing unwanted pregnancies and preventing sexually transmitted infections,” says Jessica Wood, research and project development lead at SIECCAN. “It’s really important to understand that sexual education is not just learning about safer sex and reproduction, but should be a comprehensive approach to learning about sexuality and bodies and relationships, personal and interpersonal well-being, gender and sexual diversity, and values and rights.”
Because education falls under provincial jurisdiction, sex ed experiences are known to vary widely across Canada. Approaches can differ even between classrooms in the same school, as educators have different levels of comfort and training in delivering this knowledge. This means some students get all of the details, while others are left in an unfortunate state of ignorance. And it’s not just their own openness to the topic that educators must negotiate with: the volume of anti-trans rights rhetoric can also affect the classroom.
But, according to Janani Suthan, the comprehensive sexuality education program coordinator at the Canadian Centre for Gender and Sexual Diversity, the perception that support for comprehensive sex ed is decreasing isn’t always rooted in reality. “The majority of parents, in the grand scheme of things in Canada, are supportive of their children learning about their sexual health in schools, and learning it holistically and comprehensively,” they say. “But the people that are against this are very loud and very proud about it, and are mobilizing.”
Wood also says it’s a small minority of people who are actually against students learning this critical information. Advocacy against comprehensive sex ed, led by groups like 1 Million March 4 Children and Parents for Choice in Education, are often well organized and well funded. Religious and political interest groups have a strong hand in the work of such organizations.
The spread of misinformation and disinformation about sex ed on social media has contributed to the movement. “And so when we hear about this often, it may seem as if more people are not supportive of comprehensive sex ed,” Wood explains. “We find that a lot of people actually are, but we just don’t hear that coverage as much.”
This disproportionate coverage of dissenting voices leads to the spread of myths about sexual health, sex education, and queer and trans experiences. “They don’t want youth to know about gender, [or] sex,” says Suthan. “They are fearful of youth having knowledge, of youth having skills to understand themselves better.”
If queer and trans experiences aren’t taught as part of sex ed curriculum, that leaves young people vulnerable. Since sex ed is a health and safety issue, it is reasonable to expect that all students should have equal access to it. “It’s suicide prevention, it’s mental health care. It’s everything, because a lot of issues end up linking to sexuality and relationships,” Suthan says. “It’s very much necessary for everybody.”
For those who are supportive of sex ed in the classroom, it has never been more important to speak up for young people’s right to access information. “If you can advocate, advocate. If you can’t, that’s okay,” says Suthan. “Show up for your kid.”
Sharing knowledge with young people can help to build acceptance and understanding, some of the most important parts of living a fulfilled life. “Community is where I found more information on being Two Spirit,” says Calahoo-Zeller. “You get to understand yourself and also other people… we don’t have secrets. There’s nothing to hide.”
]]>
SUNDAY, 8:01 P.M.
For five days, I revisited—with rapidly increasing frequency— the WhatsApp “last-seen” status of a man I’d met on an online-dating app. I had taken note of it at first because it was, as timestamps go, significant: Sunday, 8:01 p.m. was the exact time our most recent date had begun. At first, I figured he was just busy—and, since most people don’t use WhatsApp as a default messaging application, I figured he just wasn’t logging on because he was conducting necessary communication elsewhere. But the timestamp stuck in my head, and so I couldn’t stop checking. I started checking too much. I told people I was checking. I deleted the chat thread. I deleted his contact. I re-added his contact. The timestamp was the same. I deleted everything again.
I did this two more times before he messaged me. And the emotional release—the decrease in anxiety—was palpable.
I began paying attention to other things because up until that point, for a span of nearly a week, a timestamp had taken over my entire life.
I started online dating in the summer of 2018, after becoming single at the end of a seven-year, mostly monogamous relationship. I am also clinically depressed and diagnosed with generalized anxiety disorder. While online mediums make it easier for me to communicate with others free of the gut-punch nervousness I often experience when interacting with people in real life, mediums like Tinder and Bumble are built upon a framework of features that can spike feelings of stress, insecurity and self-doubt as much as mutually swiping right can alleviate them. The primary difference, though, is that the latter has a short half-life (by design), whereas the dull, gnawing hangover of the former can linger and build. Online dating, no more or less than any other online medium, has the potential for long-term mental harm.
Peer-reviewed studies about the mental-health implications of online dating are as prolific, now, as were similar studies incriminating social media, at the turn of the decade, when Facebook et al. consumed our collective consciousness. The news is predictably grim: A 2016 study by the American Psychological Association found both male and female Tinder users reported less satisfaction with their physical appearances than non-users, while male users reported lowered self- esteem. A 2018 survey of Match.com users found 15 percent felt “addicted” to the process of looking for a date; millennials were 125 percent more likely to report these feelings.
But the problem, I’ve observed in my peers as well as in myself, is not so much in the transactional nature of the dating apps—the inherent affirmation/rejection that accompanies a swipe right/left—but in the tiny digital breadcrumbs that surround each interaction. Take Sunday, 8:01 p.m., for instance. For the most part, dating apps require premium membership to observe when matches were last seen; the heightened visibility that often begets heightened paranoia and anxiety comes at a cost—and those who find themselves unwitting masochists to the Orwellian design of dating apps are easy monetary prey. It’s self-harm by subscription. Tinder, the Mack Daddy of dating apps, allows users to see how far they are from one another; paying to “fake” your location—to pretend you’re somewhere you’re not, either to gather matches for when you’re in town or disguise your location from a particularly nosy match—will cost you. On Bumble, seeing who has liked your profile rather than matching by accident is also pay-to- play. Feeld, an app where users are more likely to be looking for no-strings-attached physical relationships, also has a paid tier; it, among other things, allows you to hide your profile from Facebook friends who are also using the app.
There’s a commonality to each online dating application’s premium features: They essentially provide windows into the types of anxiety that are stoked once users move the conversation off the app, and into other mediums. WhatsApp’s last-seen feature—plus read receipts; Facebook’s newsfeed and mutual-friends collection; the three moving dots of iMessage; the bright blue light of a message received—of affirmation, of validation—and the dead, black screen of “I guess I’m not good enough.” Each tiny digital sign of life adds to a growing network of anxieties; a new spore in a massive, brain-blanketing fungal network of what-ifs. It’s consuming. It’s gut-wrenching. And, for the most part, it doesn’t feel like romance at all.
If none of this is ringing a bell to you, good: it may be the case that you haven’t entered the perilous arena of digital romance with a preexisting mental illness. But for those of us who have, the confluence of our always-on digital lives with the sometimes-there sparks of online romance can feel heady at best, enveloping at worst.
And since the mediums—and their anxiety-inductors— are so disparate, coping mechanisms tend to be ad hoc. They often manifest as patchwork digital desire paths: A friend of mine swears by muting notifications on dating apps as well as the text threads in which she’s engaging potential partners. She says that visiting those mental stimulators only when she chooses to lends a sense of control. Another puts his apps in a folder that’s not accessible from his cellphone home screen. Dozens of friends have told me about deleting Tinder, reinstalling it, deleting it again, opting for a different app, opting for two apps at once, deleting both, then starting anew.
Dating apps, ostensibly, exist to facilitate human connections. And this is why it’s so difficult to apply the advice often levelled at those of us who find social media anxiety- inducing—“Just delete it!”—to Tinder and its cousins. We can still keep in touch with our friends and family without the helping hand of Mark Zuckerberg; our phones still have, um, a phone function. But we aren’t speed-dating anymore. Swiping right is the new meet cute. And if you already tend toward introversion due to mental health issues, opting out of digital dating may seem tantamount to joining a convent. Otherwise, it’s a precarious tightrope walk, attempting to balance the temptation of choice, the promise of sexual freedom and the desire for romantic intimacy, with the anxiety-riddled need for order and no surprises. So what’s to be done?
Two weeks after the Sunday, 8:01 p.m. incident, I blocked that match from being able to contact me altogether. I needed to give myself the feeling of being in control. Shortly after, I spent some time with a casual partner of mine, who apologized for having recently gone quiet on me for a few weeks. He said he’d been experiencing a minor mental-health crisis, and had to take some time off. I was taken aback by his candour, at once happy that he felt safe enough to share this information with me, and embarrassed at my shock that, even in such a casual context, openness about mental wellness could be so easy.
I texted Sunday, 8:01 p.m. not long after. I told him I had no way of knowing if he’d reached out, because I’d blocked him, because my anxious brain needed a bit of a break. He hasn’t replied, and I don’t care if he does. I feel honest and I feel relieved, and this makes me feel more in control of my mental health than checking status updates and muting conversations. It feels better than pretending to feel nothing at all.
A sex addict meets another sex addict and falls in love.
Sex Addict 1 needs sex all the time, but it can be with the same person as long as
1. It’s interesting
2. The person smells good
3. They both come at least once almost every time
4. It is done in many new ways and with a sense of adventure
Sex Addict 1 knows she loves Sex Addict 2 forever. Sex Addict 2 needs sex all the time, but hopefully
1. With as many people as possible
2. In as many different ways as possible
3. In unexpected circumstances
4. Without needing to worry about anyone’s feelings
Sex Addict 2 cares about Sex Addict 1’s feelings and is constantly thinking about the lists. Sex Addict 2 also isn’t sure he believes in love – he’s never seen it at least, despite feeling the way he does with Sex Addict 1. Also how can love exist when the lists also exist?
When a Sex Addict dreams of the perfect person to love them, that person is always a Sex Addict. And, of course, at first it is perfect. Sex Addict 2 finally feels that lying does not have to be part of his addiction, that he can have sex regularly with someone he cares about and still be able to nurture his urges and have someone who will try new things, explore his fantasies, and understand his needs. Sex Addict 1 feels that sexual compatibility is probably the way to true intimacy, that the fact that she finally has someone she finds attractive, interesting, good smelling, and funny to have sex with multiple times a day must mean that they are soulmates.
One night when they are out for dinner, Sex Addict 1 congratulates Sex Addict 2 on how decent he is when they disagree—that he never yells or swears at her or even seems to get too angry. Usually, when he becomes angry or upset, he’ll verbalize his feelings instead of acting out. “I’m feeling angry,” he’ll say. “I’m hurt by what you said.” Or sometimes he’ll even break down his feelings further: “I’m not angry with you. I’m just annoyed. I’m frustrated.” Coming from a family of yelling and cursing and emotions that never seemed to go away, Sex Addict 1 finds this trait endearing in Sex Addict 2 and it makes her love grow. Sex Addict 2 says, “Well, I don’t know what we’d really have to fight about. We seem to agree on everything.”
That night they get into a fight. It is the same version of a fight that they will continue to have and that previously was a “discussion” about the fate of their relationship. Each fight comes closer to the inevitable truth: they have different items on their lists. Somehow, in deciding they are perfect for each other, Sex Addict 1 and Sex Addict 2 have fallen back into their old patterns and have been lying.
In fact, if Sex Addict 1 is honest, it isn’t sex that draws her in, or even the intimacy—it’s feeling like her whole body is being erased. She needs to be hugged, she needs to be held, she needs to be surrounded, she needs to smell parts of another human’s body. She might not even be a sex addict at all—sometimes it’s easy for her to think about other things, to let ideas be what hold her, envelop her. Sometimes she dances around the kitchen and that feels almost as good. But if her connection with Sex Addict 2 finds its basis in their mutual sex addiction, then she can never renounce her identity as a sex addict or even be more specific about what it actually is.
***
It is unclear if we can really frame the situation Sex Addict 1 and 2 find themselves in as being “A sex addict meets another sex addict and falls in love.” This is because if Sex Addict 2 doubts the very existence of love (or at least his own ability to love actively in a way that makes everyone involved feel good), it is doubtful that he has ever allowed himself to exist in the state of “being in love” or that if he has, he has not allowed himself to recognize this state as being in love, or allowed himself to exist within it before rushing off to pursue his addiction.
If Sex Addict 2 has never “been in love” with Sex Addict 1, then it is doubtful that Sex Addict 1 has ever “been in love” with Sex Addict 2. Sex Addict 1 tries to figure this situation out with her friends the way she tries to figure everything out, by speaking. She tells them about the lists. She describes the different positions she and Sex Addict 2 have used. She describes her fear of being alone and her desire to be completely encased. She gives examples of Sex Addict 2’s behaviour and asks for interpretation. She gets almost the same answer, with different diction, depending on the friend: “He doesn’t seem to be a very self-aware person. Whereas you seem to be! I’m amazed by your awareness.” Sex Addict 1 appreciates compliments during times like this, although from the details provided about Sex Addicts 1 and 2, it’s easy to see that this assessment is false.
Sex Addict 1 has not selected her friends according to the trend of picking people whom you admire professionally or want to be in some capacity, who dedicate their conversational power to the discussion of their ambitions and interests and reveal very little of their inner life.
Sex Addict 1, while admiring her friends for their talents and abilities, has chosen her friends for their compassion, creativity, and what she (as much as she can tell, being a generally poor judge of character) thinks is their good hearts. She enjoys the long hours they spend tolerating her as she talks about herself, love, and sex. But since these are fully developed people, they would also enjoy speaking about:
1. Their interests
2. Outer space
3. Animals
4. The existence of ghosts
5. New scientific discoveries
6. The upcoming election
7. Pipelines
8. A new job they may get
9. A movie they just saw
10. Their families
11. The war in Syria
12. Their health
13. A plane that went missing
14. An upcoming event that they have to go to but really don’t want to go to
15. Netflix
And get frustrated by the limited nature of Sex Addict 1’s focus. On some level, Sex Addict 1 also acknowledges that the crumbling partnership between her and Sex Addict 2 was always fairly shallow. “It’s only about attraction and pain. Why did I ever think those things are deep? They aren’t about the world, they aren’t about goals, dreams, secret desires, they aren’t about life or death. They aren’t even about the person, not really.” Her friends nod along and try to change the subject. Sex Addict 1 has exhausted her lines of support.
***
It’s hard to say what will become of Sex Addict 2. Some of their mutual friends say they see him going for walks around the city. Some say he’s learning how to be on his own. Some say he thinks about love sometimes, wonders if he’s wrong, thinks that maybe he can do it. He’s always been surprised by the way time moves around him, and maybe it’s a new season now—it’s getting colder. He blows on his hands and pushes them deeper into his pockets.
***
The world is also changing around Sex Addict 1. Perhaps this is because she is no longer seeing everything through the lens of sex. She always thought she was a pretty decent human being except when it came to sex, and then sometimes she did things that she didn’t quite mean to do. For instance, when she first met Sex Addict 2, she informed him that he was in love with her and then tried to grab his dick through his pants underneath the table, even though they were at the bar surrounded by people and he had a girlfriend. Sex Addict 1 had also been drinking, which of course didn’t help any of that behaviour, but feeling sexual like that felt like being drunk anyway, somehow uninhibited, somehow operating on instinct.
Whenever Sex Addict 1 thinks about this behaviour in isolation, she thinks that this must be the behaviour of a bad person, that it’s the addiction, but then when she turns it around and looks at it another way, it seems like most every person is at least a little like that.
Other times, it’s as if she’s separate from herself in those moments and that there is a real split in herself and that the her who needs sex is there to destroy the her who needs tenderness, the one who needs to be shielded, hugged, cared for. Sex Addict 1 has never understood why she can’t occupy both these spaces at once and thinks something must be wrong with her.
In the early morning, Sex Addict 1 goes for a run. She is trying to replace a hunger for sex with taking care of herself. Sometimes when she misses Sex Addict 2, she uses a vibrator. These sessions can last hours, and Sex Addict 1 finds that she’s able to merge sex with tenderness or at least blur the lines slightly. Not that she tries to fantasize about tenderness, but she recognizes the very act of pleasuring herself in this way is an act of tenderness, especially if it means she’s not opening herself up to Sex Addict 2 again.
As she runs in the morning, she feels the same thing—the borders of her physicality break up so that the heart that has always been a little too sore in her is released and beating and her brain is quiet and sun is staining the sky all over in pink and purple and orange.
Illustration by Rosena Fung.
]]> All too often, people with disabilities are left out of the body positivity conversation. That’s why when Andrew Gurza was asked to pose in Toronto alt-weekly Now magazine’s “Love Your Body” issue in January 2015 completely naked, he felt excited and hopeful to start a dialogue about bodies that are not typically considered beautiful. “I like playing with the fear that people place on me,” Gurza explains. In the past year, he’s done a great job at getting people to talk, be it out of fear or not. (For the sake of full disclosure, Gurza and I met online when we appeared in the same Now issue, and I’ve posed in photos promoting his work in the past.)
All too often, people with disabilities are left out of the body positivity conversation. That’s why when Andrew Gurza was asked to pose in Toronto alt-weekly Now magazine’s “Love Your Body” issue in January 2015 completely naked, he felt excited and hopeful to start a dialogue about bodies that are not typically considered beautiful. “I like playing with the fear that people place on me,” Gurza explains. In the past year, he’s done a great job at getting people to talk, be it out of fear or not. (For the sake of full disclosure, Gurza and I met online when we appeared in the same Now issue, and I’ve posed in photos promoting his work in the past.)
Gurza, a disability awareness consultant since 2012, has made it his mission to get Canadians to stop, think about, and discuss how people with disabilities are portrayed in society—including their sexuality and desires. Since the launch of his website, AndrewGurza.com, in January 2015, his message is slowly making its way to folks both in Canada and across the world.
People with disabilities face a number of challenges. One hurdle Gurza has faced is that society largely views disabled folks as undesirable or asexual beings. “Sex and disability make most people uncomfortable because they haven’t had the chance to see disabled people sexualized in a way that gives them agency over their bodies and their experiences,” he says. As a result, Gurza has spent considerable time over the past four years crafting his voice. He has worked tirelessly to reclaim words such as “disabled” and “crippled.” Through social media and his blog, he provides readers with insight on the real disabled experience. “It is never really seen as something normative and accepted at all,” he says.
In February 2015, Gurza launched Disability After Dark, a weekly podcast dedicated to disability and sex. He talks frankly about everything from sex and sexuality, desire, devotion, accessibility, sexual identity, and queer culture, and often invites guests on the show to share their experiences. In a recent episode, “Accessing Anal,” Gurza discusses the inaccessibility of anal sex to a person with disabilities, using himself as the example. Its open and honest format has paid off: The podcast has reached nearly 6,000 downloads since its inception.
Gurza also speaks across North America about disability, on topics ranging from body image issues to long-term care. “Being a disability awareness consultant, I want people aware of what the disabled experience—what my experience—as a queer disabled man feels like,” he says. “I want to bring everyone into my experiences and give them a seat at my table.”
It’s hard to deny that while Gurza’s voice is valuable for the disability community in general, it is extraordinarily valuable and necessary in the queer community. As a queer man, he’s aware of the “homonormative ideal,” which assumes that all queer people must conform to certain ideal beauty standards or fit certain stereotypes. From being flamboyant and feminine to having huge muscles and a beard, these ideals have plagued Gurza throughout his life, and he has been confronted with an incredible amount of ableism and discrimination from within the community. “I’d be lying if I said it didn’t hurt,” he says. “It burns each and every time.” From being asked blatant questions about his body (“Does your penis work?”), to being unable to access queer spaces both physically and emotionally, much of this has fueled Gurza’s work. “I use the tough parts [of my own life] to bolster my mission of shining a light on the reality of disability,” Gurza says.
Gurza has embraced his status as a kinky cripple who has worked overtime to dispel the myths that plague those who have disabilities. “What I am trying to do in my work is shine a light on what disability is really like for me,” he explains. “There are days when living as a disabled person isn’t awesome, and no matter how much positivity you use, nothing will change that.” He believes that by showing Canadians the emotional side of disability, they will have a better understanding of how disability affects folks in all aspects of their lives. Most recently, a parent who listened to Gurza’s podcast wrote in to say that because of him, they now had the words to talk to their disabled teenager about sex. “When I read that, I was bowled over. I mean, it doesn’t get much better than that,” he says.
This year, Gurza is challenging himself to something different: he’s in the midst of writing a book proposal based on his blogs and planning a lecture series based on his podcast series. “I want my voice to be among the many disabled people, to bring disability that much closer to the mainstream,” he says. Gurza may just be the voice to end the stigma and make you look at disability differently
]]>
When hooking up with partners I meet through online dating apps, I keep my expectations low. More often than not, hookups from Tinder, the smartphone app that allows you to swipe through potential suitors within a certain geographic range, don’t give me an orgasm, let alone an epiphany about my sexuality. It takes time for a new person to learn the quirks of my body and how to please me, just as it takes time for them to get to know my mind.
So I was surprised when my one-night stand on a trip to Minneapolis taught me something I didn’t know about myself.
We started off with me going down on him. I was happy to do that and to keep doing that, but midway through his stream of generic dirty talk, he proposed doing something more. I lifted my head, miffed by the interruption, and pondered his question. Then I shrugged, and said, “Nah.”
The truth is that good ol’-fashioned intercourse doesn’t turn my crank anymore. As I talked with other folks my age about this, I noticed I wasn’t the only one disillusioned with conventional sex. Penetrative intercourse, or penis-in-vagina sex (PIV)—once thought of as a standard, expected sexual act—seems to be on the decline.
It’s no secret that millennials aren’t reproducing at the same rate as our predecessors. A 2012 study by the Urban Institute found that twenty-something women’s birth rates had dropped more than 15 percent since 2007. It’s unsurprising that this drop coincided with the 2008 financial crisis: a generation coming of age in a decimated economy would naturally be pickier about which expensive choices we make. Increasingly, we can’t find work in our fields, so it follows that we might avoid the sexual act likeliest to land us with a baby-shaped financial commitment. Heart-pounding money anxiety isn’t exactly an aphrodisiac.
But fear of consequences historically hasn’t been much of a sexual deterrent, especially for the young and horny, as countless unplanned pregnancies and STI transmissions can attest. If we’re less interested in intercourse, it’s not only because of fear, but also because our desire for the act itself has decreased.
We can chalk some of this up to the sexual revolution and women’s sexual liberation. That process has been ongoing since the 1960s, when feminism and the introduction of the birth control pill made it easier and more acceptable for women to pursue sex outside of marriage and for purposes other than reproduction. Now, fewer young women are content to just “lie back and think of England.” Studies indicate that anywhere from half to three-quarters of women need clitoral stimulation in order to reach orgasm—and while PIV sex boasts plenty of fun features, consistent clit contact isn’t one of them. Although penetration feels fantastic for many women, it lacks orgasmic potential for many of us. Millennials of all genders are more clued in to this crucial information than any other generation. If we want an orgasm, we’re likelier to ask for it or to make it happen ourselves.
But you’d be surprised how many men sneer at a woman who actively claims her own orgasm. I’ll always remember the time I pulled out a clitoral vibrator during intercourse with a new partner. When he felt the vibrations transmitted through my body, he wrinkled his nose and declared, “That feels weird!” I know many women who’ve been similarly chastised by men for trying to pleasure themselves. One friend of mine started touching herself while hooking up with a hot Irish boy, who then rendered himself much less hot by sneering, “What the hell are you doing?” My friend had never been so embarrassed during sex in her life. Since having an orgasm during PIV can be both difficult and stigmatized for women, it’s reasonable if we favour acts that make us come more easily and let us relax into receiving pleasure.
It’s not only women who are falling out of love with PIV. Many men I know—including my Minneapolis hookup—seem reluctant to pursue PIV with their partners like they used to. They approach intercourse as if it’s a favour they’re ambivalently performing for their partner’s benefit, rather than a fun activity they’re excited about. It’s not that these men are generally unenthused about sex: many are passionate about oral and digital sex. But hand them a condom and get into position and their erections will wilt.
Intercourse is commonly characterized as a “performance” for men, with articles and advice columns sharing tips for boosting “endurance” and “stamina.” The PIV narrative still centres around toxic masculinity, even as our sexual culture shifts toward gentleness and mutuality. It’s unsurprising that men would get nervous about an act cloaked in so much dogma: last longer, stay harder, perform better. Using their mouths or hands on partners, and having partners do the same to them, is a much lower-stakes situation for men and may allow them to relax and enjoy themselves in a way PIV doesn’t.
Condoms, too, make intercourse unappetizing for some. Some men report stunted sensitivity when sheathed in latex. Many women, including me, choose not to use hormonal birth control because of its side effects, so condoms are often the contraception of choice—and many dudes will choose no PIV at all over sex with a condom.
Millennials, in general, aren’t big on sexual scripts. We still watch porn and read erotica: the under-35 age group makes up 60 percent of visitors to Pornhub.com, according to the website, and the average age of users on erotic fan-fiction hotbed Archive of Our Own is 25 years old, reports a recent survey. That said, most of us know real-life sex isn’t as formulaic as it is in those mediums. This may have to do with the “queerification” of our culture. Fewer than half of teens identify as exclusively straight, according to a 2016 study done by the J. Walter Thompson Innovation Group. Even dead-set heterosexuals these days are more exposed to non-normative sexual identities than ever, through their friends and the media they consume. Queer sex has always been more freeform than straight sex, allowing for (and even celebrating) variations in desire. While it’s a stretch to say that hetero sexploits are in any way “queer,” even the straightest of straight millennials are more open to non-traditional sex than heterosexuals have ever been before. And if that means they’re rejecting the go-to sex act, intercourse, on the basis that it just doesn’t stoke their carnal flames, more power to ’em.
As for me, my attitude toward PIV is perpetually in flux. By itself, it offers little appeal to my kinky, queer heart, and I find other, non-traditional sexual acts more fun and more pleasurable. Growing up in the 21st century has taught me that any approach to sex is valid as long as it’s safe, consensual, and mutually enjoyable. Millennials might throw out the old rulebook of sex, but we still like playing the game.
]]>The store has now moved to an all-ages format, eliminating the sexually explicit videos and magazines, says Taylor in an e-mail to This.
Venus Envy has locations in Ottawa and Halifax. The shops are trans-affirming. The stores also sell books and health products around safer sex, in addition to toys, and also offerworkshops on sex education. As its website says, “Anyone who’s turned off by traditional sex shops will find us a welcoming and informative place to get cool and sexy stuff.” On October 9 Venus Envy started a Pay it Forward Campaign, offering free binders and gaffs (similar to a jock strap) through their shops. This is possible through donations (which you can make here). “We’ve had a lot of interest in our new Pay It Forward campaign that was sparked by this whole kerfuffle,” says Taylor.
A former This intern, Hillary Di Menna is in her second year of the gender and women’s studies program at York University. She also maintains an online feminist resource directory, FIRE- Feminist Internet Resource Exchange.
]]>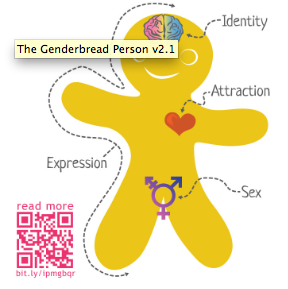
Sam Killermann’s Genderbread Person
On April 29, B.C.’s Maple Ridge-Mission MLA voted against allowing people to change their gender designation on their birth certificate if they haven’t had gender reassignment surgery.
Bill 17 was first introduced March 10. Maple Ridge-Mission MLA Marc Dalton voted against Section 115, saying, “My concern is it might lead to more self-acceptance issues with young people.” In the past, Dalton has called homosexuality a moral issue, like pornography, adultery, gambling and abortion as well as promoting a church that aims to cure homosexuality in the legislature.
Perhaps Dalton should read GLAAD’s tips for allies of transgender people: “It wouldn’t be appropriate to ask a non-transgender person about the appearance or status of their genitalia, so it isn’t appropriate to ask a transgender person that question either.”
Gender and sex can be independent from each other. As the World Health Organization explains, “sex” refers to a person’s biological and physiological characteristics, where “gender” is about socially constructed roles; what a society sees as masculine or feminine behaviours. Things like sexual orientation are not dependent on an individual’s gender; a transgender person, for instance, is not automatically gay.
Dalton doesn’t get it, and probably never will. Gender, like sexual orientation, is not a choice. As teacher and staff liaison for the gay-straight alliance at Thomas Haney Secondary, Kathryn Ferguson, says: “Thank you, Mr. Dalton, for reminding me why we do need gay-straight alliance groups in the public school system.”
]]> Inside the silence behind sex, dating, and disability
Inside the silence behind sex, dating, and disability
It took less than 30 seconds for the date to go from promising to very bad. After some online chatting, Steve* was excited to meet Kayla, the 24-year-old law clerk he connected with on Plentyoffish. They’d decided on Toronto’s Bull and Firkin Pub, one early evening in August 2012. He spotted her first: strawberry blonde hair, pouty lips—even more attractive in person. Steve, a 27-year-old publicist who has cerebral palsy, uses a pair of canes or a wheelchair for mobility. Tonight, he brought the chair. He smiled at her and headed toward the table. Approaching, he saw Kayla’s calm expression change. She looked puzzled, he says, like a lost child. Her eyes darted down to his wheelchair.
Steve wondered why she looked confused: his dating profile clearly showed him seated in a wheelchair. Plus, it was Kayla who had messaged him first. Maybe she didn’t see his picture? Maybe she thought he was in a Halloween costume? Within two minutes of meeting each other, Steve knew the “maybe” didn’t matter—it was clear, he says now, that Kayla was no longer interested. Her eyes wandered as they chatted. She smiled at her phone more than him. In between sips of his Miller Genuine Draft, Steve asked Kayla the regular get-to-know-you first date questions. She responded with short answers. He says he wanted to sway Kayla’s perception of him, but nothing charmed her. Soon, he just wanted to leave, but didn’t want to be rude. The date lasted 45 uncomfortable minutes, before they decided to split the bill. As Kayla chatted on her phone, Steve backed his wheelchair out from the table and waved goodbye. She waved back limply, still talking on her phone.
She never mentioned his wheelchair. Neither did he. That’s what disappointed him the most: he understood why she was uninterested without her having to say anything.
While growing up, Steve was smothered with attention. “I don’t wanna talk shit or whatever,” he says with a laugh, “but I was a really cute kid. Like really, really cute—just darling.” Based on his own childhood experiences, Steve observes that people tend to be more receptive and doting to kids with disabilities. Now as a grown man with a boyish face and icy blue eyes, Steve says people are generally nice to him. When he goes out, strangers tell him it’s cool that he’s just a guy living his life, which is true. Sometimes, however, he feels like people look at him the way they look at mascots at football games.
As for dating, it’s a minefield of challenges: Before worrying about what to say or what to wear on a date, Steve—like many people with disabilities—feels he has to convince a woman that he’s a human being too (see: Kayla). He must convince them, he says, that his physical disability doesn’t negate his ability or desire to date and have sex—not such an easy task considering the challenges.
Here’s an appalling revelation: Many people believe those with disabilities cannot, will not, and should not contribute to the future of the human race, writes Tobin Siebers, a professor at the University of Michigan, in an essay published in Sex and Disability in December 2011. Such people believe those with disabilities are not capable of reproduction, but if they do manage, the expectation is that the results will be tainted. The ability to reproduce, adds Siebers, is also what society believes makes someone a “quality” human being. Someone who is infertile or physically and mentally unfit for sex is considered “less than human.”
It’s no wonder, then, that a culture of silence has cocooned the disability community. “Sexuality is often the source of our deepest oppression and pain,” says Anne Finger, an American disability issues writer and activist who became disabled after contracting polio as a toddler. Finger says it’s easier for people with disabilities to talk about—and formulate strategies for changing—discrimination in employment, education and housing than it is to delve into their exclusion from sexuality and reproduction. It’s even less easy to talk about the possible need for assistance during sex, the stigma, or even how to overcome disparities in able-bodied and non-able-bodied couples. Sexual rights are not a priority in the disability rights movement, says Finger; it’s creating an image of “the able disabled.”
Unfortunately, the refusal to talk about sex and disability has created plenty of misinformed assumptions—such as the ones Siebers cites and more—and a widespread denial of sexualities and rights. In 2006, about 4.4 million Canadians reported having a disability according to Human Resources and Skills Development Canada statistics. The three most reported disabilities were lack of mobility, pain, and reduced agility among people aged 15 and over. It’s hard to believe none of these millions of people desire sex.
 In 2011, Tim Rose and his wife, Natalie Sanborn, founded The Rose Centre for young adults with disabilities. The centre’s mission, in part, is to promote discussion and awareness on disability and sexuality (its secondary goal is to promote positive focus on disability, relationships and sexuality in the general public). Rose, 28, has cerebral palsy spastic quadriplegia while Sanborn is able-bodied. They met through a mutual friend before Rose moved to England in 2011 for his studies. The distance didn’t stop the romance: Now, the two are newlyweds. Rose says they often get strange looks and questions. “She’s been asked if she’s my mother or my nurse,” he says. Still, the couple says they choose to remain light-hearted. Instead of getting angry, they joke that Sanborn will never have to carry groceries—she can just hang them on the back of Rose’s wheelchair. This same positive attitude led to the Rose Centre; with no resources to help navigate dating with disabilities, the two decided to create their own. The centre doesn’t have a permanent space (yet), but it hosts monthly discussion nights and social events at Ryerson University.
In 2011, Tim Rose and his wife, Natalie Sanborn, founded The Rose Centre for young adults with disabilities. The centre’s mission, in part, is to promote discussion and awareness on disability and sexuality (its secondary goal is to promote positive focus on disability, relationships and sexuality in the general public). Rose, 28, has cerebral palsy spastic quadriplegia while Sanborn is able-bodied. They met through a mutual friend before Rose moved to England in 2011 for his studies. The distance didn’t stop the romance: Now, the two are newlyweds. Rose says they often get strange looks and questions. “She’s been asked if she’s my mother or my nurse,” he says. Still, the couple says they choose to remain light-hearted. Instead of getting angry, they joke that Sanborn will never have to carry groceries—she can just hang them on the back of Rose’s wheelchair. This same positive attitude led to the Rose Centre; with no resources to help navigate dating with disabilities, the two decided to create their own. The centre doesn’t have a permanent space (yet), but it hosts monthly discussion nights and social events at Ryerson University.
Rose says people of all backgrounds and disabilities attend the centre’s events and meetings. “A lot of people who come say they’ve never had anyone to talk to about this,” he adds, “They always keep things internal.” Many attendees lack knowledge and experience in dating. Some have no experience in, as the colloquial term goes, “making out.” When it comes to knowledge about dating, and such romantic and sexual relationships, he says, many attendees are stunted in their knowledge. And, perhaps embarrassed to talk about it. In situations like these, Rose and six volunteers can start the conversation by talking about their own personal struggles—like how Rose disliked having sex until he “redefined” sex and made it comfortable for himself—and ways to overcome them.
It doesn’t help that sex is such a taboo subject, period. Because of this people want to be careful about what they say, says Demian Brown, a Toronto psychotherapist. That includes people with disabilities and those without. The spectrum of disabilities, and the unique needs, experiences, and challenges, are vast. Perhaps it goes without saying that cerebral palsy isn’t the same as muscle atrophy, and muscle atrophy isn’t the same as spina bifida. People don’t want to look like they don’t know enough about the issue, says Brown. They fear appearing insensitive, ignorant or bigoted. So they clamp up. “If there’s stigma in general, it wouldn’t be easier for one person with a disability to talk about sex to another person who has a different disability,” says Brown. He says it takes someone brave enough to talk about these issues, first, before communities—and society as a whole—will join the conversation, and grow it outward.
When it comes to the dating world, this sense of the taboo can translate in weird, demeaning ways. Helena*, a 33-year-old Master’s student at the University of Toronto with spinal muscular atrophy, is engaged to her partner of two years. She and her fiancé have talked about having a child one day. It may be difficult—“I would probably require a surrogate and genetic testing before we are able to have one”—but Helena is happy. It wasn’t always that way. Back in her 20s, she says, many guys saw her as “just” a friend or a sexual partner—but not somebody they could form a relationship with.
Helena felt she had to decide if she wanted to be alone and not experience intimacy—or if she should take a chance, meet men online and explore her sexuality. She chose to embrace her sexuality. Mostly, she met men online. She and whoever she messaged would express upfront their interest in having sex. But she also looked for romantic partners. Sometimes she went on dates to develop a relationship, sometimes it was for “other experiences.” Helena thinks of sex as a natural and beautiful part of human experience that should be celebrated. “I never felt ashamed of it. I’ve always been an explorer of life experience.” Helena says she had several sexual partners as a result, but very few relationships throughout her 20s. The men she met while in university wanted to have sex with her out of curiosity or saw her as “an experience.” Helena doesn’t mind. She thinks maybe they craved a new experience, like how she wanted different sexual experiences to learn more about herself.
This is not uncommon. Many people are sexually attracted to people who have physical disabilities—because of their disability. They are called “devotees.” Unsurprisingly, devotees are a wildly controversial topic. Among the many concerns are: whether these type of relationships exploit people with disabilities; whether it turns people into a fetish object; and also what messages are being sent when the disability is put first. Raymond J. Aguilera is a disabled California-based writer who writes on queer and disability issues. He says while there are some devotees who may fall into the “concern” category, there are disabled men and women who choose to participate in these relationships to a devotee. Although he says it’s impossible to say devotees are “good” or “bad”, he believes it’s sex-negative that most of the scholarship in this area portray devotees as predatory and exploitive.
More often, though, this outside culture of silence is fed by the seemingly unshakeable misconception that people with disabilities are asexual. They can’t have sex; they don’t want to have sex. Steve, who says he has a decent amount of sexual experience, says people assume his penis is shrivelled or doesn’t work. “It’s almost like old people having sex,” he says. It’s easy [for people] to convince themselves that ‘they’ don’t do it or ‘it’ doesn’t work.” In one stereotype, mainstream society dismisses people with physical disabilities as undesirable or incapable sexual partners.
Rose knows all about this misconception. Many visitors who come to The Rose Centre say some people assume they’re asexual or incapable of having sex. “In my experience,” he says, “people with disabilities are some of the horniest people I’ve met.”
Sometimes, though, mobility can be an issue—and sex can be physically impossible without personal assistance. In Canada, the profession of personal support workers (PSWs) is unregulated. Support workers are hired directly by clients and work in the client’s home, or they’re hired by agencies, hospitals, and facilitated living buildings. In all settings, their job is to assist clients with daily chores such as cooking, showering and dressing. Many agencies do have policies stating that personal support workers shouldn’t assist their clients with anything related to sex. Due to the unregulated profession and flexibility to create their own policies, though, some agencies or individual personal support workers may choose to provide sexual assistance. This is most often the case if a support worker and client develop a strong enough relationship that the worker is comfortable assisting in sex-related activities, such as manoeuvring their clients in sexual positions for their partner. “It happens under the table,” says Steve, “They become friends.”
But it doesn’t always end well. Brown, the Toronto psychotherapist, did a placement in a mental health hospital in Whitby in 2004. While there, he heard about two support workers—not at his hospital—who had helped their patients with sex and were subsequently fired. Brown and his colleagues realized if they didn’t address these issues, some patients would be at risk. There could be patients living with serious mental or physical conditions consenting to sex with other patients who were more mentally aware or physically able for sex—this breached issues of safety and ethics. Brown used that insight to develop the groundwork and research to create a policy, guided by the belief that patients had the right to engage in consensual sex with other patients. In the end, workers in the hospital were, in theory, allowed to help their patients during sexual encounters if they strongly needed assistance—an issue that, he says, never arose while he was there.
The policy outlined how workers can handle these situations. Long-term patients who expressed desire and consent to have sex would be led to conjugal rooms supplied with condoms. Though not officially part of the policy, workers could assist patients out of wheelchairs, manoeuver them in positions or supply them with birth control if needed. Before the policy was created, discussion on sex and disabilities was often discouraged or ignored. Differing moralities of each individual contributed to the fear of being rejected for their personal views. “No one wants to expose their sexual views,” says Brown. “If you talk about patients’ sexualities, you’re implicitly talking about yourself.”
Rose has consulted PSWs to assist him and a past girlfriend, who also had disabilities, for sexual encounters. “It can be awkward and a little weird,” he says, “but that’s just part of the relationship.” It’s a healthy attitude to have, especially considering that, as Rose says, the topic of assistance during sex is rarely discussed. People need help, he adds, but they feel weird asking for it—it’s not the same as asking for help cooking, and few guidelines have been put in place to make it so. The thought of refusal can be devastating, and it happens. Helena has heard several stories where workers denied service to clients who needed help during sexual encounters. “Even in long-term monogamous relationships with consenting adults,” she says, “service is refused because the personal support worker is uncomfortable.” Because of varying policies and moral beliefs, not all workers are trained or comfortable enough to handle these situations.
Steve deactivated his profile on Plentyoffish last February. Due to medical reasons, he says he didn’t go out much because of pain in his back and joints. Dating fell low on his list of priorities. Mostly, he didn’t think most women were capable of dealing with his chronic pain and “other crazy things” that many people don’t understand. At the time, it seemed easier to just avoid relationships.
But then he met Crystal*, a petite, brunette woman, in April 2013 at a networking seminar at The House of Moments, an art gallery and restaurant. Three weeks later, Crystal asked Steve out on a date. In June, the two became a monogamous couple. Like most fresh couples, they had a lot to learn about each other. Steve learned that Crystal has mild cerebral palsy. He also noticed her quirks, like how she sometimes bites her bottom lip when she thinks or when she bobs her head rhythmically to her favourite songs. Their relationship is getting serious, but they’re taking it slow. They’re savouring their time together. As for the sex: Steve says it’s both fantastic and plentiful.
]]>Plus, in our pursuit to compile the alternative answer to mainstream media’s not-so-progressive body and sex coverage, we want to hear from you! We’ll be printing our favourite reader answers to the following three questions:
Tell us about your “first time.” At This, we love us some diversity. So please, please, please help us cover the full range of “aw” to “awkward” with stories that also show the full scope of sexuality, gender and ability.
So you already know 125-gazillion ways to pleasure “him.” But how do you pleasure yourself?
Oh, sex education. Share your best (worst?) sex ed stories with us. Was your class helpful, quaint, terrible? We want to hear it all, from ha-ha to horrible.
Email your answers to [email protected] or leave them in the comments sections. We don’t need your name—it’s completely anonymous if you want it to be!
]]>